Free Printable Health Care Surrogate Form
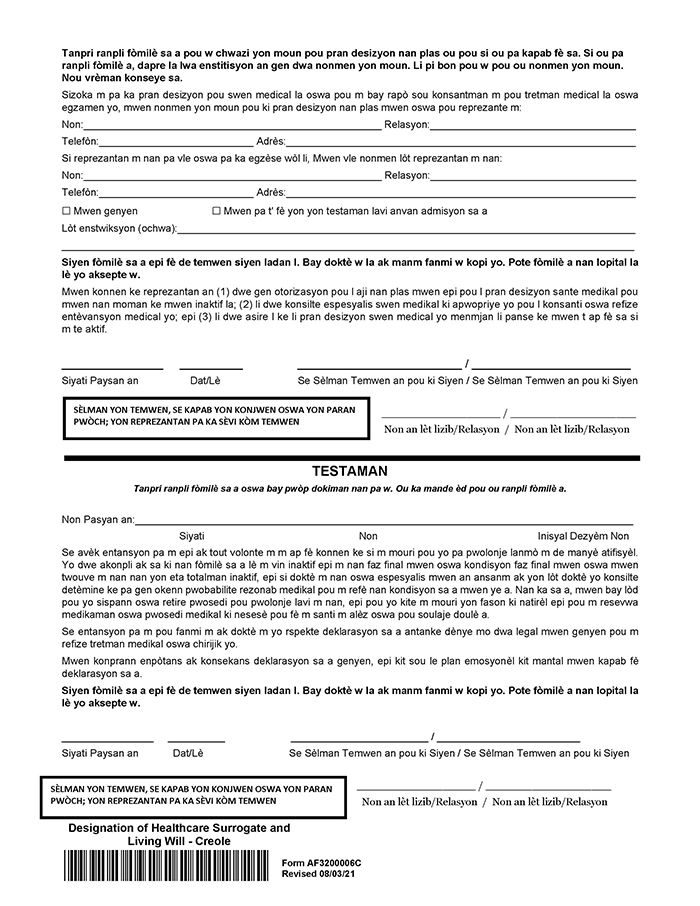
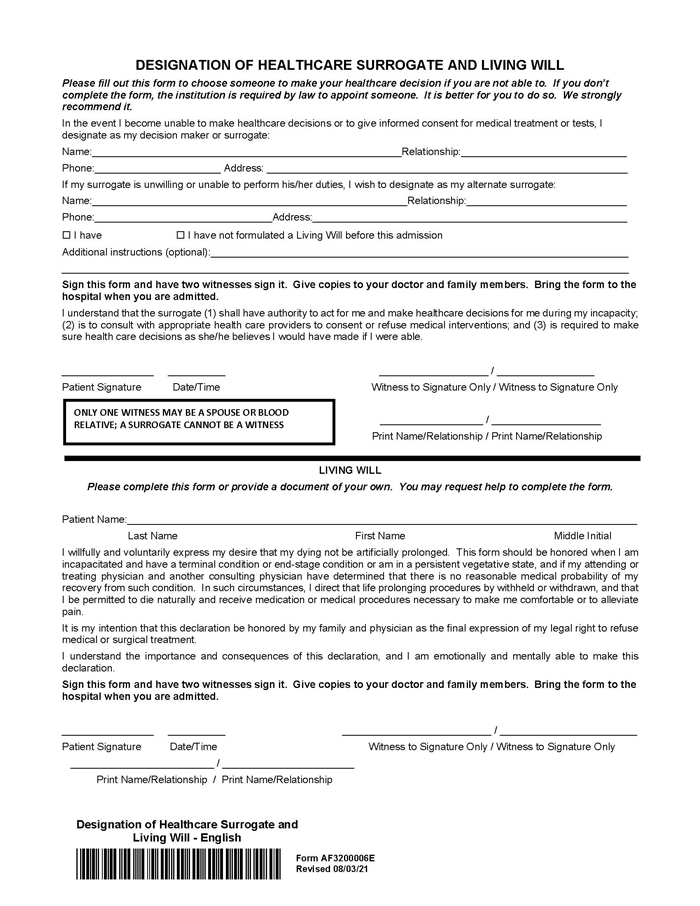
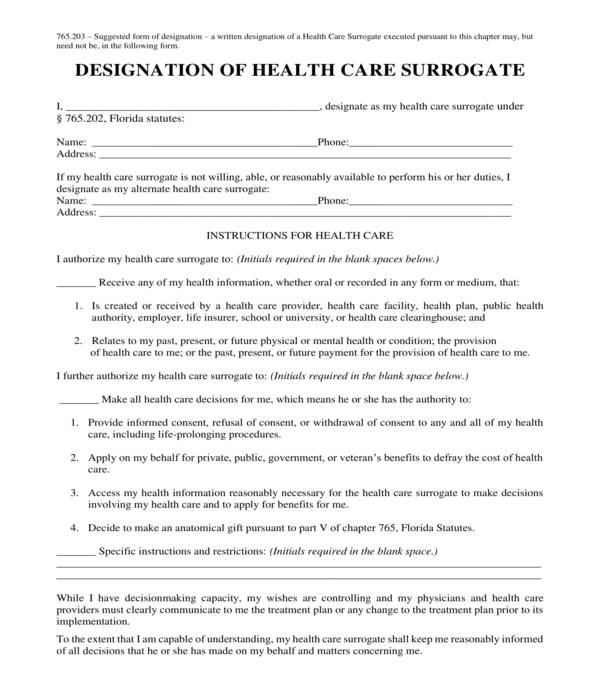
Free Printable Health Care Surrogate Form - Download a free printable form to designate a health care surrogate under florida law. The form allows you to authorize your surrogate to access your health information, make health care decisions,. Access my health information reasonably necessary for the health care surrogate. Or apply for public benefits to defray. If i am unable to communicate or make my medical decisions, my health care surrogate (hcs) will: Under florida law, designation of a health care surrogate should be made through a written document, and should be signed in the presence. Download a free printable form to designate your health care surrogate in florida. Any competent adult may also designate authority to a health care surrogate to make all health care decisions during any period of incapacity. I fully understand that this designation will permit my designee to make health care decisions and to provide, withhold, or withdraw consent on my behalf; I fully understand that this designation will permit my designee to make health care decisions and to provide, withhold, or withdraw consent on my behalf; I fully understand that this designation will permit my designee to make health care decisions and to provide, withhold, or withdraw consent on my behalf; Apply on my behalf for private, public, government,. Access my health information reasonably necessary for the health care surrogate. Download a free printable form to designate a health care surrogate under florida law. Instructions for my health care surrogate: How do i designate a health care surrogate? Designation of health care surrogate*[ (and hipaa release authorization)]* in the event that i, _____[aka], have been determined to be. • talk to my health care team and. Apply on my behalf for private, public, government, or veterans’ benefits to defray the cost of health care. I fully understand that this designation will permit my designee to make health care decisions and to provide, withhold, or withdraw consent on my behalf; Access my health information reasonably necessary for the health care surrogate. The form allows you to authorize your surrogate to access your health information, make health care decisions,. To apply for public benefits to defray. Designation of a health care surrogate this health care surrogate designation form will help the healthcare team speak to the person you trust to speak. If i am unable to communicate or make my medical decisions, my health care surrogate (hcs) will: I fully understand that this designation will permit my designee to make health care decisions and to provide, withhold, or withdraw consent on my behalf; Designation of a health care surrogate this health care surrogate designation form will help the healthcare team speak. I fully understand that this designation will permit my designee to make health care decisions and to provide, withhold, or withdraw consent on my behalf; Download a free printable form to designate your health care surrogate in florida. Designation of a health care surrogate this health care surrogate designation form will help the healthcare team speak to the person you. Under florida law, designation of a health care surrogate should be made through a written document, and should be signed in the presence. How do i designate a health care surrogate? The form allows you to authorize your surrogate to access your health information, make health care decisions,. To apply for public benefits to defray. Instructions for my health care. How do i designate a health care surrogate? Designation of a health care surrogate this health care surrogate designation form will help the healthcare team speak to the person you trust to speak on your behalf when you are no longer. • talk to my health care team and. If i am unable to communicate or make my medical decisions,. Download a free printable form to designate your health care surrogate in florida. I fully understand that this designation will permit my designee to make health care decisions and to provide, withhold, or withdraw consent on my behalf; Access my health information reasonably necessary for the health care surrogate. Apply on my behalf for private, public, government,. The form gives. Download a free printable form to designate your health care surrogate in florida. Designation of health care surrogate*[ (and hipaa release authorization)]* in the event that i, _____[aka], have been determined to be. The form allows you to authorize your surrogate to access your health information, make health care decisions,. Or apply for public benefits to defray. The form allows. If i am unable to communicate or make my medical decisions, my health care surrogate (hcs) will: • talk to my health care team and. The form gives those that complete it peace of mind knowing that their health care choices will be respected when (or if) they are unable to communicate them due to a medical condition. The form. If i am unable to communicate or make my medical decisions, my health care surrogate (hcs) will: Any competent adult may also designate authority to a health care surrogate to make all health care decisions during any period of incapacity. Designation of health care surrogate*[ (and hipaa release authorization)]* in the event that i, _____[aka], have been determined to be.. Download a free printable form to designate your health care surrogate in florida. Download a free printable form to designate a health care surrogate under florida law. To apply for public benefits to defray. Under florida law, designation of a health care surrogate should be made through a written document, and should be signed in the presence. I fully understand. To apply for public benefits to defray. To apply for public benefits to defray. The form allows you to authorize your surrogate to access your health information, make health care decisions,. How do i designate a health care surrogate? Apply on my behalf for private, public, government,. I fully understand that this designation will permit my designee to make health care decisions and to provide, withhold, or withdraw consent on my behalf; The form allows you to authorize your surrogate to access your health information, make health care. Fully understand that this designation will permit my designee to make health care decisions and to provide, withhold, or withdraw consent on my behalf; Apply on my behalf for private, public, government,. Designation of health care surrogate*[ (and hipaa release authorization)]* in the event that i, _____[aka], have been determined to be. The form gives those that complete it peace of mind knowing that their health care choices will be respected when (or if) they are unable to communicate them due to a medical condition. If i am unable to communicate or make my medical decisions, my health care surrogate (hcs) will: Any competent adult may also designate authority to a health care surrogate to make all health care decisions during any period of incapacity. Under florida law, designation of a health care surrogate should be made through a written document, and should be signed in the presence. Instructions for my health care surrogate: I fully understand that this designation will permit my designee to make health care decisions and to provide, withhold, or withdraw consent on my behalf;
Healthcare Surrogate Form Fill Out, Sign Online and Download PDF
FREE 5+ Health Care Surrogate Forms in PDF
Designation Of Health Care Surrogate Florida Printable Form

Free health care surrogate form Fill out & sign online DocHub
Does A Health Care Surrogate Form Need To Be Notarized Printable
FREE 5+ Health Care Surrogate Forms in PDF

(DOC) ADVANCE DIRECTIVES LIVING WILL and DESIGNATION OF HEALTH CARE
FREE 5+ Health Care Surrogate Forms in PDF
Free Printable Health Care Surrogate Form

Health Care Surrogate Worksheet —
I Fully Understand That This Designation Will Permit My Designee To Make Health Care Decisions And To Provide, Withhold, Or Withdraw Consent On My Behalf;
What Is A Health Care Surrogate?
Or Apply For Public Benefits To Defray.
If My Health Care Surrogate Is Not Willing, Able, Or Reasonably Available To Perform His Or Her Duties, I Designate As My Alternate Health Care Surrogate:
Related Post: